Education & Community
Oral Health Initiative: Rosarito, Mexico
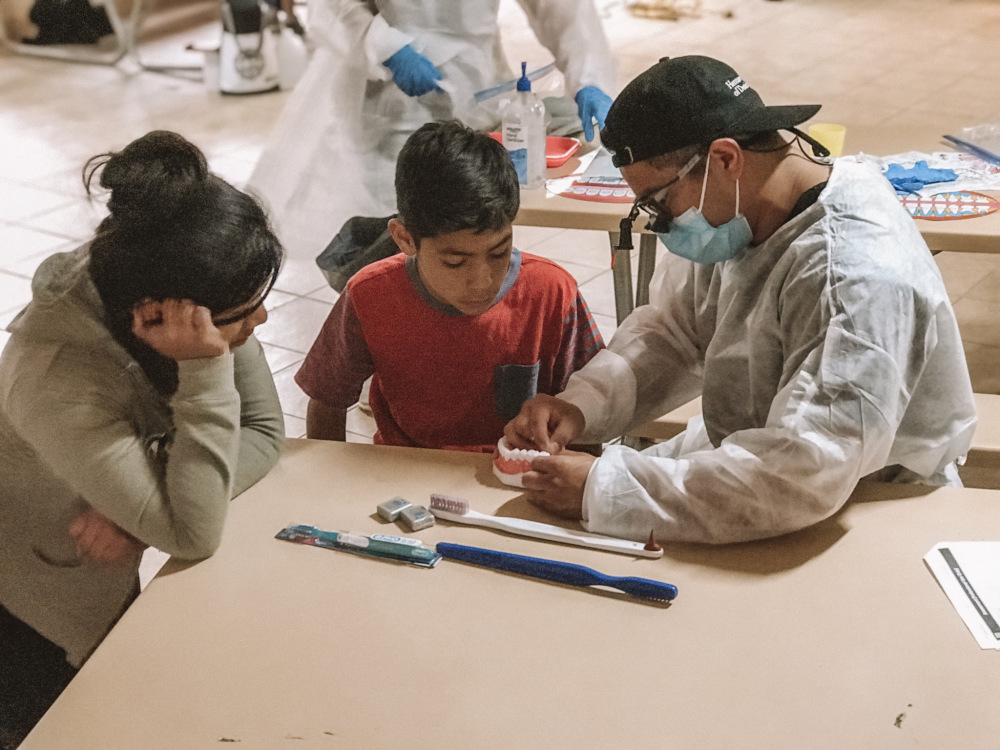
Oral Hygiene Initiative (OHI): Established as an oral health educational program in 2017 by the Rotary Club of Newport Beach it has now grown to include clinical preventive services. OHI DH volunteers provide prophy/scaling, fluoride treatments, sealants and hygiene instructions to underserved children in underdeveloped areas.
Rosarito, Mexico: We served children in 9 different orphanages over a span of 3 days. Many came from unfortunate home situations and had experienced abuse and/or poverty.
Assessment & Planning: Working with a representative from each of the 9 orphanages the total number of children and their age range were estimated. A budget based on the number of children and cost of supplies was then prepared. 12 volunteers from my senior dental hygiene class were recruited and then what was thought to be an ideal sequence for the clinic flow based on the number of children and number of volunteers was developed.A patient Consent Form was developed and translated into Spanish. The form included demographic and medical information along with a section to document the child’s oral health. For children over age 11, an assessment of how untreated dental caries impact their daily life activities was included.
Industry Partners: Premier Dental donated a generous supply of fluoride varnish and prophy paste.
Provided Services: Overall, preventive care to 203 children was provided, approximately valued at $88,000. Services included:
- 203 Screenings, Fluoride treatments and Oral Hygiene Instructions
- 142 Prophy’s (plaque removal)
- 56 Scaling (calculus/stain)
- 127 Sealants



Evaluation and Limitations: The program was an overall success in terms of the care we provided and our ability to demonstrate that we could set up a dental hygiene clinic almost anywhere! All 9 locations were different and our team was able to adapt their set-up to each one. Analysis of our data revealed that 53% of the children had untreated decay and subsequently were referred for follow-up care.
Limitations and planning advice: Upon arrival I was asked to split the volunteer DHs into 2 groups. This meant dividing and repacking supplies and coordinating volunteers on the spot. Next time I will make sure to ask if we are expected to work in small groups so I know how organize the volunteers and pack the supplies.Each group went to 2-3 orphanages a day, which meant we had to pack up clinic supplies and air compressors, using too much of our valuable time. After day 1, we stopped using the air compressors and will not bring them in the future.
We had more adolescent patients than expected, consequently the next time I will bring more toothbrushes than needed so that we have enough supplies for all ages. (Better to have too much than not enough!)
Time was an issue. The clinic flow was disrupted due to splitting the team into two groups and the paperwork more extensive than needed. Also, the Consent Form did not include permission for using photos and will be added before my next program.